Leg Fractures
Fracture Treatment at Children’s Mercy
Femur fractures
The femur, or thigh bone, is the largest and also one of the strongest bones in the body. It forms both the hip and knee joints. Fractures can occur at any location along the bone, although factors like your child’s age, the fracture location, and alignment can all impact the treatment plan.
The femur requires a lot of energy to fracture, so these fractures typically occur as the result of accidents such as car crashes, contact sports or falls from a height. Any femur fracture in an infant or toddler who is not yet walking is concerning and may be a sign of child abuse. Occasionally, a femur fracture can heal in a shortened position or have some overgrowth while healing, so your doctor may suggest monitoring leg lengths for several years following the injury.
Hip fracture
A fracture of the upper portion of the femur is considered a hip fracture and can be treated with a soft harness or brace in infants and toddlers. Older children and adolescents will likely require a hip spica cast or potentially surgery, depending on the location and severity of the fracture.
Femoral shaft fracture
A femoral shaft fracture is a break in the midportion of the bone. It is typically treated with a hip spica cast with or without closed reduction (setting the bone without surgery). In some cases, this type of fracture may require surgical correction using flexible nails, rigid nails or plates and screws. Older children or children with more severe fractures are more likely to require surgery due to the reduced potential for their body to naturally remodel and reshape the bone.
Distal femur fracture
These fractures occur just above the knee and frequently involve the growth plate in this area. These fractures can be treated in a long-leg cast, but if they involve the growth plate, your child’s doctor will need to monitor the leg in the future due to the potential for growth disturbance.
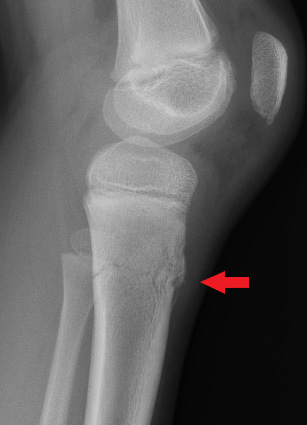
Examples of femur fractures


X-rays of the left knee. Image A shows the front view (anteroposterior); image B shows the side view (lateral). The red arrows show a Salter-Harris II fracture of the thigh bone (distal femur). A Salter-Harris Type II fracture is a fracture that goes through the thicker part of a long bone and the growth plate—a layer of tissue near the ends of a child’s bone—but doesn’t affect the end of the bone.
Tibia fractures
The tibia, or shin bone, is one of the two bones in the lower leg that forms both the knee and ankle joints. Tibia fractures can occur both with high-energy injuries or with any sort of twisting injury. Any portion of the tibia can be fractured, but the middle portion (or shaft) is the most common area to sustain a fracture. Treatment varies based on your child’s age and the fracture location and alignment. Fractures involving the upper portion of the tibia closer to the knee require a long-leg cast, whereas fractures to the middle to lower portions closer to the ankle might be treated with a short-leg cast or even a walking boot.
Proximal tibia fracture
A proximal tibia fracture is a fracture of the upper end of the tibia near the knee. This most commonly occurs in young children and is sometimes referred to as a trampoline fracture, since this is a common mechanism of injury. While it can occur when a small child is jumping and bouncing on a surface individually, more often than not, this fracture happens when multiple people are jumping together. When bigger, older children or adults are jumping together with smaller children, this causes the smaller, lighter children to get “double bounced” and land from a high jump or land such that there is minimal recoil in the trampoline. These fractures are treated with 3-4 weeks in a long-leg cast which they can typically walk in. Future visits may be necessary if the fracture involves the growth plate.
Examples of proximal tibia fractures

X-rays of the left knee. Image A shows the front view (anteroposterior); image B shows the side view (lateral). The red arrows show a fracture of the shinbone just below the knee (proximal tibia).
Tibial shaft fracture
A tibial shaft fracture is a fracture that occurs through the middle portion of the tibia. This type of fracture can occur with falls or direct force onto the lower leg, such as collisions in sports or heavy objects falling on the leg. A specific type of fracture known as a toddler’s fracture occurs here and usually only requires a small twisting force on the leg such as when someone trips or slides on a surface and falls.
The treatment is based on the alignment of the fracture and your child’s age. Many of these types of fractures can be managed without surgery. These are typically placed in either a cast or a boot and some require the bone alignment to be adjusted slightly with sedation prior to placing in a cast. Weekly visits for x-rays during the initial phases of care can be helpful to ensure the fracture continues to be aligned correctly. For the first several weeks in the cast, your child should not bear weight on the injured leg. After some time, your care provider will tell you when weight bearing is allowed. It can take a minimum of 2-3 months from the time of the injury before the bone is healed adequately to return to normal activities.
Examples of tibial shaft fractures


X-rays of the left lower leg bones (tibia/fibula). Image A shows the front view (anteroposterior); image B shows the side view (lateral). The red arrows show a shinbone (tibia) shaft fracture.
Distal tibial fracture
A distal tibial fracture is a fracture that occurs in the lower portion of the tibia near the ankle. These fractures commonly involve the growth plate and therefore can require additional imaging such as a CT to check the alignment and better help to guide treatment. If alignment is acceptable, they are treated with a short-leg cast or a boot, but typically your child will need to wait a few weeks to walk on the injured leg. If the fracture involves the growth plate, your care provider will discuss future monitoring with x-rays to ensure normal continuation of growth.
Examples of distal tibial fractures

