Abstract: Baseline quality improvement culture assessment for centers participating in the T1D Exchange QI Collaborative
Ann Mungmode1; Kristina Cossen2; J. Sonya Haw3; Grace Nelson4; Priyanka Mathias5; Nicole Rioles1; Donna Eng6; Ori Odugbesan1; Meredith Wilkes7; Mark Clements8; Sarah D. Corathers9; G. Todd Alonso10; Osagie Ebekozien1,11 on behalf of the T1D Exchange QI Collaborative
1T1D Exchange, Boston, Massachusetts, USA; 2Childrenʼs Healthcare of Atlanta; 3Grady Memorial Hospital, Emory University; 4Le Bonheur, University of Tennessee; 5Albert Einstein College of Medicine; 6Helen DeVos Childrenʼs Hospital; 7Mount Sinai Health System; 8Childrenʼs Mercy Hospital, University of Missouri; 9Cincinnati Childrenʼs Hospital Medical Center; 10Barbara Davis Center, University of Colorado; 11University of Mississippi School of Population Health
Background/Objective: The T1D Exchange Quality Improvement Collaborative (T1Dx-QI) is a learning health system of type 1 diabetes clinics with a shared mission to improve health outcomes using quality improvement (QI) methods. However, clinics join the T1Dx-QI with variable levels of QI experience. This abstract summarizes baseline survey results across 33 T1Dx-QI clinics.
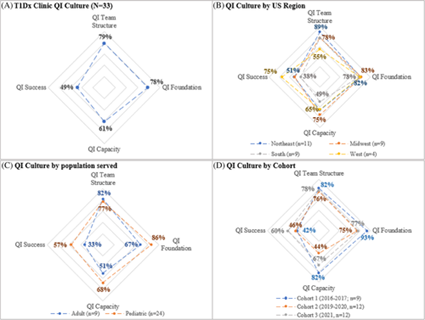
Methods: Clinics complete a 20-question QI Culture self-assessment as part of their orientation process to evaluate experience using QI methodology to improve clinical practice. The assessment measures QI culture across four evidence-based areas: QI Team Structure (team roles); QI Foundation (data collection and training); QI Capacity (use of QI tools); and QI Success (scaling up small tests). A QI coach validates the preliminary results of the self-assessment by semi-structured interview. Results were analyzed for all clinics, by population served, US geographic region, and when the clinics joined the T1Dx-QI.
Results: Overall, T1Dx clinics had strong QI Team Structure and QI Foundation (Figure 1, Panel A). Cohorts varied significantly (38%, Panel B) in QI Capacity. Pediatric sites were assessed stronger in three of four areas compared to adult sites (Panel C). Finally, results varied by US region significantly in three of four areas, differing by 23%-37% in QI Team Structure, QI Capacity, and QI Success (Panel D).
Conclusions: Cohort 1 clinics joined the T1Dx-QI with a higher baseline QI culture than subsequent Cohorts, indicating T1Dx-QI network maturity and ability to train sites with variable pre-existing capacity. QI networks can use this assessment framework to customize clinic-specific QI coaching and support skill growth.