Poor Weight Gain: What's the Diagnosis?
Visual Diagnosis - May 2023
Column Author and Editor: Joe Julian, MD, MPHTM | Hospitalist, Internal Medicine-Pediatrics; Clinical Associate Professor, Internal Medicine & Pediatrics
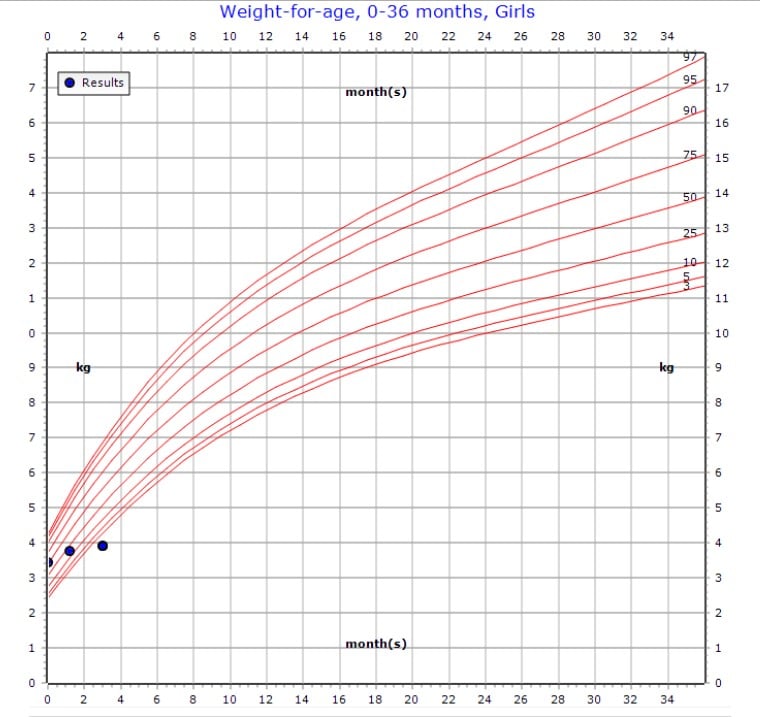
A 3-month-old female is admitted directly to the hospital for further evaluation of poor weight gain.
Patient was born at 40 weeks’ gestational age via spontaneous vaginal delivery. Birth weight was 3.46 kg (7 lbs, 10 oz). Prenatal course was uncomplicated and maternal screening labs were appropriate. Patient passed congenital heart disease screening prior to nursery discharge. She had breastfeeding jaundice which eventually resolved and did not require phototherapy. Newborn screen was within normal limits.
There was some initial decrease in weight after birth, but birth weight was regained appropriately. Mother states that weight plateaued about one month ago. Patient started child care recently, but refused a bottle at all (ingesting only 1-1.5 oz/feed, if any). Mother worked with her pediatrician and tried formula, fortifying breast milk, bottle changes, and nipple changes in addition to breastfeeding at home. Her home regimen is generally 20 minutes of breastfeeding at a time. Mother fed breast milk via bottle in order to quantify feeds and found that her baby took about 3-3.5 oz every two to three hours. Mother was also coming to the child care during the day to feed her due to the concerning lack of weight gain.
Patient has appropriate wet diapers and three to four stools per day which are yellow and seedy. She has recently started having perioral cyanosis with prolonged crying and becomes sweaty during prolonged feeding attempts and while crying. No other recent illnesses, coughing, gagging, vomiting or rashes. Father and mother are both healthy. Patient is an only child.
OBJECTIVE
Heart rate 128, respiratory rate 34, and oxygen saturation 100% on room air.
Weight 3.93 kg (0.09%ile), length 56.5 cm (6%ile), head circumference 36.5 cm (0.74%ile).
Comfortable, no acute distress.
Anterior fontanelle open/soft, clear sclera, no tongue tie, normal palate.
Mild increased work of breathing with subcostal retractions.
Lungs are clear to auscultation bilaterally with adequate aeration, pectus carinatum present.
Regular rate and rhythm, 3/6 systolic murmur heard best anteriorly, 2/6 early diastolic murmur.
Abdomen is soft and non-tender, no organomegaly.
Extremities are warm and well perfused, normal fingers/toes.
Unremarkable female genitalia that is appropriate for age.
Skin is loose with diffuse loss of subcutaneous fat noted.
Tone is mildly diminished but can briefly hold head up.
QUESTION
What is the most likely cause of this patient’s poor weight gain?
- Congenital heart disease
- Poor feeding technique by caregivers
- Vascular ring
- None – weight changes are appropriate
ANSWER
A. Congenital heart disease
This patient’s weight changes are certainly abnormal – she has dropped off the growth chart entirely. While the exam is consistent with a malnourished infant, the heart exam (3/6 systolic murmur, questionable diastolic murmur) and history (cyanosis and diaphoresis with agitation/feeding) are concerning for a cardiac etiology.
The congenital heart disease screening algorithm (available here) is designed to screen for critical congenital cardiac conditions that cause early hypoxemia and can lead to early death if untreated (e.g., “ductal-dependent lesions”). These conditions include truncus arteriosus, transposition of the great arteries, tricuspid atresia, tetralogy of Fallot and pulmonary atresia. Passing the cardiac screening in the nursery does not rule out the presence of other structural cardiac anomalies.
The caregivers and pediatrician made multiple attempts to adjust the feeding regimen and the quantified volumes seem reasonable enough to promote ongoing growth. However, there do appear to be some issues with feeding (most notable at child care) which are likely related to an underlying cardiac condition.
Presenting symptoms of vascular rings vary and can include respiratory and esophageal symptoms. Poor oral intake is a non-specific symptom for a vascular ring and it would not explain the diaphoresis with feeding, the perioral cyanosis while crying, or the heart murmur present on exam. Of note, vascular rings are not infrequently associated with congenital cardiac anomalies.
CASE CONTINUED
An echocardiogram was obtained that showed hypertrophic cardiomyopathy with severe concentric left ventricular hypertrophy. The left ventricular cavity was almost completely obliterated during systole. Right ventricular hypertrophy with a prominent muscle bundle causing turbulence was also present. The patient was transferred to the cardiology service where a genetic workup was started.
SOURCES:
DynaMed. Failure to thrive in children. Accessed May 2023.
Kemper AR, Mahle WT, Martin GR, et al. Strategies for implementing screening for critical congenital heart disease. Pediatrics. 2011;128(5):e1259-e1267.
Tang MN, Adolphe S, Rogers SR, Frank DA. Failure to thrive or growth faltering: medical, developmental/behavioral, nutritional, and social dimensions. Pediatr Rev. 2021;42(11):590-603.
See all the articles in this month's Link Newsletter
Stay up-to-date on the latest developments and innovations in pediatric care - read the April issue of The Link.