Wide World of Vaccines
May 2021
What Have We Learned from COVID-19 Pandemic Projections that are Used to Plan Public Health Responses in the U.S.?

Author: Christopher Harrison, MD | Professor of Pediatrics, UMKC School of Medicine | Clinical Professor of Pediatrics, University of Kansas School of Medicine
You may wonder where policymakers, government agencies and public health officials get projections about the upcoming and ongoing COVID-19 pandemic outcomes with regard to expected hospitalizations and deaths, e.g., between now and Sept. 1 when schools are hopefully going to re-open. One source is a group that has a website we can all access. (https://covid19scenariomodelinghub.org/viz.html). This is the COVID-19 Scenario Modeling Hub.
This source is an independent panel of experts who mostly volunteer their efforts to calculate a consensus from other expert scientific groups, with each group having submitted their projections, including deaths and hospitalizations, over the near term and long term. The projections are based on different interacting variables such as vaccine uptake, the blend of circulating variants, and use of non-pharmaceutical interventions (NPI – e.g., social distancing, hand hygiene and masks).
The COVID-19 Scenario Modeling Hub group calculates an overall “ensemble” projection for cumulative hospitalizations and deaths by calculating the median from all proposed algorithms (usually 6-12 algorithms) and provides a range of values that estimate cumulative numbers at differing levels of certainty (no uncertainty up to 95% uncertainty).
This past month the hub group released a report where they had two dependent variables, i.e., % use of NPI and % vaccine uptake, while holding all other variables constant. In other words, if everything else stays the same, what will be the impact of reducing social restrictions and increasing vaccine uptake in parallel? Their goal was to give a reasonable projection if new variants do not come to predominate, and vaccine supplies/demand remain at mid-April levels. Figure 1 and 2.
Definitions/assumptions used in projections:
- NPI:
- “Moderate” if the evolving rollbacks in the public’s actual use of social mitigation (masks and social distancing and avoiding large public gatherings) end up preventing 50% of the possible transmissions that would occur if no NPI were used.
- “Low” if the rollbacks end up preventing 20% of possible transmissions.
- Vaccine uptake:
- High – near 90% uptake.
- Low – max of 75% uptake.
- Recovery from infection of any severity due to any SARS-CoV-2 strain confers complete and permanent immunity (best-case scenario).
- Variant proportions will not shift over time.
- For each of the three vaccines with EUA so far, vaccine effectiveness (VE) will be 95% for Moderna and Pfizer, and 70% for Johnson & Johnson; VE values will continue unchanged indefinitely (also best-case scenario).
Bottom line: Even with the above-defined close to best-case-scenario, there will almost certainly be an ongoing summer surge. The summer surge will increase deaths and in a worse (not worst) case scenario reach almost 800,000 deaths (18,000 new deaths/month) nationally (Figure 1) by Sept. 1. This mimics the severe numbers seen regionally in Arizona and Michigan in April 2021 and those occurring now in some international venues (India, Brazil, Sweden). However, our future could be better (with better-than-expected vaccine uptake and immune-evading variants not becoming dominant) or it could be even worse (stalling vaccine uptake and immune-evading variants exploding in numbers).
What is clear from real-world data is that mild infections with the original Wuhan strain offer insufficient protection from the immune-evading variants (Brazil, South Africa, Sweden and India prove that), so the original hypothesis that we could return to normal by letting most people get mild infection was bogus. Vaccine-induced immunity and immunity from moderate-severe illness are more protective. My advice – vaccine is a better way to go than getting sick with SARS-CoV-2. So, every eligible person should get the vaccine. And, until we get >75% of the U.S. immunized, including children (P.S. 12-15-year-olds are now eligible to receive Pfizer’s COVID-19 vaccine following FDA Emergency Use Authorization on May 10), the unvaccinated and vaccinated need to follow the now relaxed new CDC guidelines updated May 15, 2021 (https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html) on masks (fully immunized need masks only in select situations even indoors and around travel and dense crowds), while still following local and state mandates plus workplace rules).
Despite what some regional U.S. politicians are saying, THIS IS NOT OVER YET. While we can have more confidence that things can soon become more normal, we need to hang tight for two to three more months and the CDC will continue to gradually give us safe guidance on reopening America. If we follow that advice, the worse- or worst-case projections for hospitalizations/deaths will not come true. Let’s not give new variants a chance to take hold in the U.S.
Figure 1.
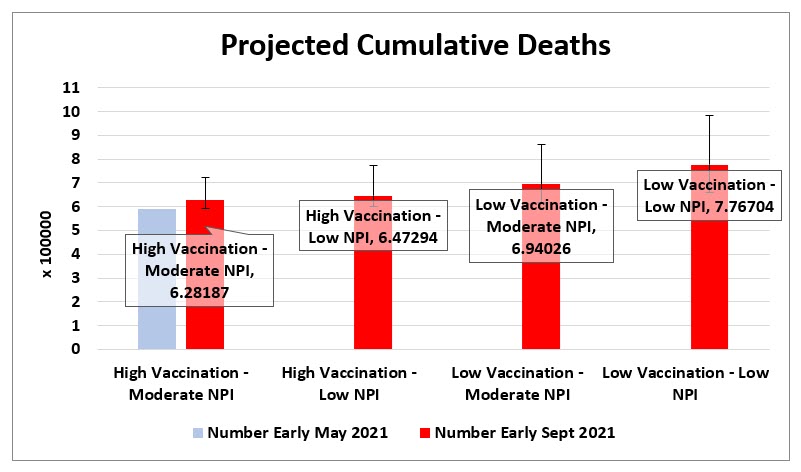
Figure 2.
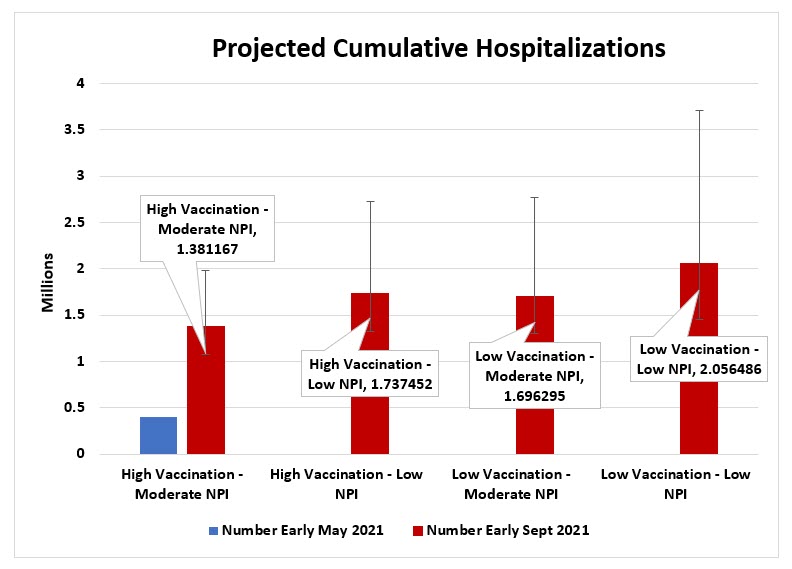
Both figures adapted from data at https://covid19scenariomodelinghub.org/viz.html