What's the Diagnosis?
July 2021
Visual Diagnosis

Author: Laura Plencner, MD | Pediatric Hospital Medicine | Associate Professor of Pediatrics, UMKC School of Medicine

Column Editor: Joe Julian, MD, MPHTM, FAAP | Hospitalist, Internal Medicine - Pediatrics | Assistant Professor, Internal Medicine and Pediatrics, UMKC School of Medicine
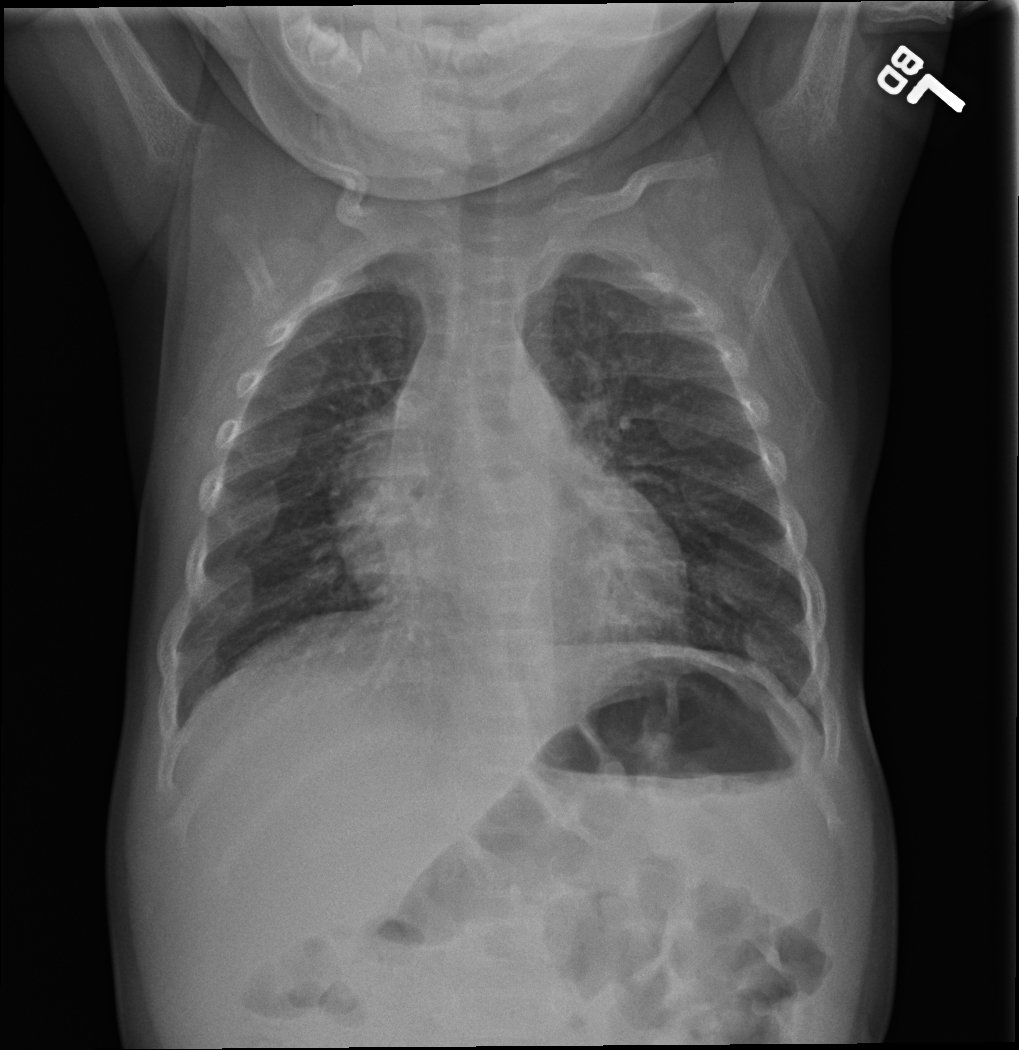
A 10-month-old boy presents for one day of fever and a few weeks of congestion and runny nose. He has had two days of emesis and diarrhea. He was born at full term via uncomplicated vaginal delivery. He has no previously diagnosed medical conditions but mother notes that his weight had not been increasing as expected at his last well-child examination. He breastfeeds for 5-15 minutes every 2-4 hours and takes formula when mother is not home. He is offered a variety of table foods but does not eat a large amount. He takes no medications or supplements. On exam he is noted to be febrile and have congestion but no tachypnea or retractions and his lungs are clear to auscultation bilaterally. A chest radiograph is obtained.
Of the following, what is the etiology of his chest radiograph findings?
A. Bacterial pneumonia
B. Child abuse
C. Hodgkin's lymphoma
D. Vitamin D deficiency
Answer: D. Vitamin D deficiency
The radiographs show diffuse demineralization, bilateral cupping and fraying of the bilateral humeral metaphyses, and multilevel osseous expansion of the anterior ribs at the costochondral junction (rachitic rosary) consistent with rickets. The radiographic findings associated with bacterial pneumonia would include focal pulmonary consolidation. Chest radiographic findings associated with physical child abuse in an infant can include posterior rib fractures caused by compression of the chest during squeezing or shaking and not anterior osseous expansion. While Hodgkin’s lymphoma can present with weight loss and fever, radiographic findings include mediastinal mass which is often large at the time of presentation.
The patient was found to have hypocalcemia, hypophosphatemia, elevated parathyroid level, and elevated alkaline phosphatase and was diagnosed with nutritional vitamin D deficient rickets based on a history of breastfeeding without vitamin D supplementation.
Rickets is caused by abnormal bone mineralization at the growth plates and abnormal structure of the bones due to inadequate calcium and phosphate. Normal bone growth is a balance of chondrocyte proliferation and vascular invasion of the growth plate to convert to bone spongiosa. Calcium and phosphorus are necessary for the growth plate to mineralize and when calcium or phosphorus stores are inadequate, the growth plate thickens and is not mineralized and the chondrocytes become disorganized. These abnormalities lead to the radiographic findings of thickened and cupped metaphyses, as well as enlargement of the costochondral junction seen in the anterior ribs. Additional clinical features can include delayed closure of the anterior and posterior fontanelles, bowing of the femur or tibia, altered gait, bone pain, poor growth, hypoplastic dental enamel and delayed motor milestones.
The most common cause of rickets is nutritional vitamin D deficiency and inadequate calcium intake. Risk factors include exclusive breastfeeding without vitamin D supplementation, dark pigmented skin, and less sunlight exposure due to being born in winter. Laboratory findings of vitamin D deficient rickets include hypophosphatemia, elevated parathyroid hormone level, and either low or normal calcium level. Treatment includes replacement of vitamin D and ensuring adequate calcium and phosphorus intake. Following treatment, improvement is seen in many of the bone deformities although short stature can be a long-term complication.
References:
- Carpenter T (2020). Overview of rickets in children. In Wolfsdorf JI and Hoppin AG (Eds.) UpToDate. Accessed online on 15 June 2021. Available from: https://www.wolterskluwer.com/en/solutions/uptodate.