State-of-the-Art Pediatrics
September 2022
ERCP: How to Get Into Those Pipes

Author: Nadia Ibrahimi, MD | Pediatric Gastroenterologist | Medical Director, Pancreas Center | Assistant Professor of Pediatrics, UMKC School of Medicine

Column Editor: Amita Amonker, MD, FAAP | Pediatric Hospitalist | Assistant Professor of Pediatrics, UMKC School of Medicine
ERCP (endoscopic retrograde cholangiopancreatography) is a well-established advanced endoscopic technique used with adults in the diagnosis and treatment of biliary and pancreatic disorders. ERCP is performed less frequently in children compared with adults in part because of lower rates of biliary calculus and pancreaticobiliary malignancy. However, with the rise in pediatric obesity, the incidence of choledocholithiasis has increased, as has the incidence of acute and chronic pancreatitis and, subsequently, the need for endoscopic intervention.
The first ERCP in an infant was reported by Waye in 1976. This report was quickly followed by descriptions of the diagnostic potential of ERCP in children in the late 1970s and was subsequently followed by multiple retrospective case series demonstrating the therapeutic benefit of ERCP in this patient population.1
What is ERCP and how is it performed?
ERCP combines the use of endoscopy and fluoroscopy to diagnose and treat pancreaticobiliary problems. The procedure is done under general anesthesia with a side-viewing duodenoscope that is passed through the pylorus into the second part of the duodenum to visualize the ampulla of Vater. The ampulla is then cannulated into the common bile duct and/or the pancreatic duct, which are then visualized with fluoroscopy. Interventions including sphincterotomy, stone extractions, dilation or stent placement can then be performed.
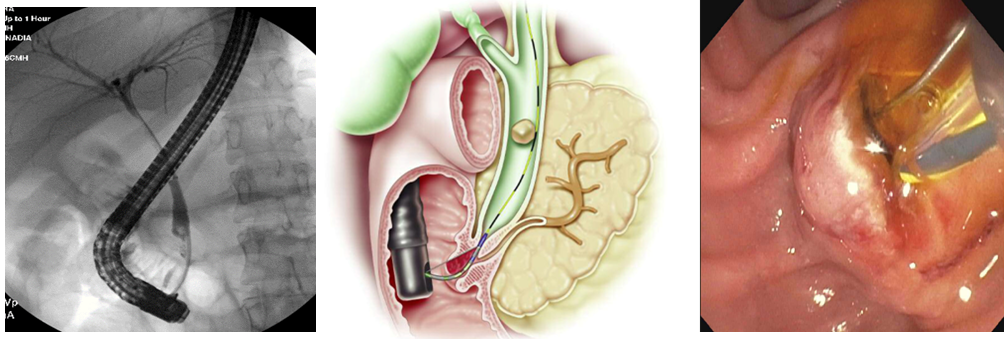
Center image courtesy of Boston Scientific Corporation
When is ERCP needed?
Since the advent of magnetic resonance cholangiopancreatography (MRCP) and other imaging modalities including endoscopic ultrasound (EUS), ERCP is now considered to be mainly a therapeutic procedure and is rarely used for diagnostic purposes alone.
The most common clinical scenarios in which ERCP is undertaken in the pediatric population are pancreaticobiliary and include the following1:
- Biliary scenarios
- Management of choledocholithiasis
- Management of biliary strictures, typically benign and seen after liver transplantation or in the setting of primary sclerosing cholangitis
- Management of post-cholecystectomy or post-liver transplant complications including bile leak or biliary strictures
- Preoperative evaluation of choledochal cyst and management of acute obstruction when present
- Preoperative evaluation of pancreaticobiliary maljunction
- Investigation of neonatal cholestasis
- Investigation of biliary pathologic abnormality of unclear cause when results of less invasive imaging modalities are equivocal or unavailable
- Pancreatic scenarios
- Management of chronic pancreatitis, with the goal of improving pancreatic drainage (removal of stones, dilation/stenting of strictures)
- Management of pancreatic divisum with minor papillotomy
- Investigation of recurrent acute pancreatitis of unclear cause
- Management of pancreatic duct leak, typically encountered in setting of abdominal trauma
- Management of pancreatic pseudocyst via transpapillary approach
- Investigation of pancreatic ductal pathologic abnormality of unclear cause when results of less invasive imaging modalities are equivocal or unavailable
Is ERCP safe?
Complication rates following ERCP are between 3% and 10%. Complications include pancreatitis, infection, hemorrhage and perforation, with the most common complication being post-ERCP pancreatitis, followed by bleeding and infection (both less than 1%).2 Major complications are rare. In general, complication rates of ERCP in infants and children seem to be similar to those in adults.3
Can ERCP be performed at children’s hospitals?
Special expertise in performing ERCP in infants and children is not widely available. In centers in which this expertise is available, ERCP is often appropriate and should be the preferred modality for treating patients with pancreaticobiliary disorders as it can prevent the need for more invasive alternatives, including percutaneous transhepatic cholangiography with catheter placement or major abdominal surgery.
Studies have shown that ERCP can be safely performed by an appropriately trained pediatric gastroenterologist in a pediatric facility with a good technical and therapeutic success rate and adverse event rate as compared to adult ERCP.4
Children’s Mercy Kansas City has been performing pediatric ERCP since March 2021.
References:
- Fox VL, Werlin SL, Heyman MB. Endoscopic retrograde cholangiopancreatography in children. Subcommittee on Endoscopy and Procedures of the Patient Care Committee of the North American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr. 2000;30(3):335-342.
- Usatin D, Fernandes M, Allen IE, Perito ER, Ostroff J, Heyman MB. Complications of endoscopic retrograde cholangiopancreatography in pediatric patients; a systematic literature review and meta-analysis. J Pediatr. 2016;179:160-165.e3.
- Keil R, Drábek J, Lochmannová J, et al. ERCP in infants, children, and adolescents—different roles of the methods in different age groups. PLoS One. 2019;14(1):e0210805.
- Troendle DM, Barth BA. ERCP can be safely and effectively performed by a pediatric gastroenterologist for choledocholithiasis in a pediatric facility. J Pediatr Gastroenterol Nutr. 2013;57(5):655-658.