Outbreaks, Alerts and Hot Topics
April 2022
When Sore Throat Becomes Emergent: Deep Neck Infections

Author: Smit Shah, MD |Emergency Medicine | Clinical Assistant Professor of Pediatrics, UMKC School of Medicine | Education Assistant Professor of Pediatrics, University of Kansas School of Medicine

Column Editor: Angela Myers, MD, MPH | Director, Division of Infectious Diseases | Professor of Pediatrics, UMKC School of Medicine | Medical Editor, The Link Newsletter
Viral infections are the most common cause of sore throat (80%), followed by group A streptococcus (20%). Infrequently, sore throat can indicate a potentially life-threatening condition. The focus of this article is to discuss acute recognition of retropharyngeal abscess (RPA), peritonsillar abscess (PTA), and bacterial tracheitis in a primary care clinic setting.
Anatomically, the clinically important deep neck spaces include (from anterior to posterior) retropharyngeal space, “danger” space, and prevertebral space. These potential spaces are separated by thin layers of fascia that allow rapid progression to airway compromise, necrosis of surrounding structures, and contiguous spread to other compartments such as the mediastinum.1
Retropharyngeal space extends from the base of the skull to the posterior mediastinum, and contains two chains of lymph nodes draining the nasopharynx, adenoids, posterior sinuses, middle ear and eustachian tube.2 As a result, half of RPA cases are associated with antecedent upper respiratory tract infection.3 Because these lymph nodes regress by puberty, RPA is most commonly found in children between 2 and 4 years of age.3 When sore throat is present in a febrile, ill-appearing child with signs of obstruction of the upper aerodigestive tract, RPA should be considered. Neck stiffness, especially with extension of neck, torticollis, neck swelling, unilateral oropharyngeal bulge and dysphagia are the most common presenting symptoms.1
Peritonsillar abscess is the most common deep neck infection in children and adolescents.2 Usually, it is a result of progression of tonsillitis or pharyngitis to peritonsillar cellulitis (phlegmon) to PTA. The typical presentation includes severe unilateral sore throat, fever and a muffled (“hot potato”) voice. Trismus is present in almost two-thirds of patients and can be the distinguishing factor from severe pharyngitis or tonsillitis.4 Anatomically, the abscess can be found as a bulge protruding asymmetrically between the two palatal arches abutting an inflamed tonsil. As a result, uvular deviation away from the affected side is often visualized.
Bacterial tracheitis is most common in the first six years of life with a mean age of 5 at diagnosis.5 Although rare, it is thought to be a superinfection of viral tracheobronchitis due to its highest incidence in the fall and winter coinciding with seasonal epidemics of influenza, respiratory syncytial virus and parainfluenza virus.2 Presentation in a child with a native airway is that of a toxic-appearing child with stridor, sudden high fevers, prodromal upper respiratory infection, hoarse voice and respiratory distress. Drooling and tripoding, hallmarks of epiglottitis, are not present.2
The evaluation of all the above serious entities includes laboratory testing for signs of infection, as well as complete blood counts and inflammatory markers (e.g., C-reactive protein), lateral neck X-ray and CT scan if available in the office in stable patients, and urgent consultation of ENT and/or anesthesia after securing airway if warranted. Although PTA is a clinical diagnosis without need for CT, CT is often obtained prior to surgery to determine the extent of disease and appropriate surgical approach. Treatment typically requires admission with intravenous antibiotics and, potentially, surgical drainage.
In summary, a combination of fever, sore throat and respiratory distress should alert a pediatrician to assess for rare but serious conditions. For a child under age 5 with neck stiffness and these symptoms, a pediatrician should consider RPA. For older children and adolescents with muffled voice and trismus, a pediatrician should consider PTA. For a toxic-appearing child under 6 with prodromal URI, a pediatrician should consider bacterial tracheitis.
Figure 1. PTA (CT scan images)
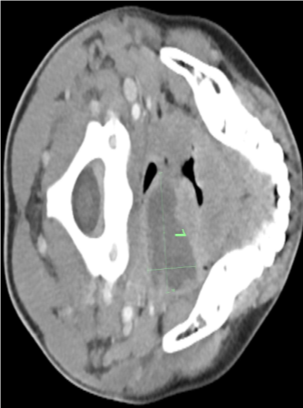
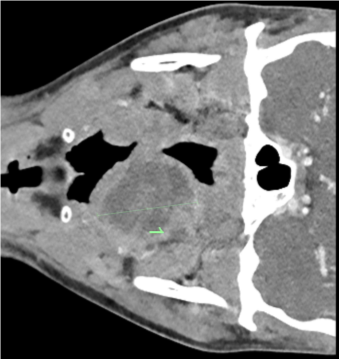
Table 1. Comparisons between RPA, PTA and bacterial tracheitis
|
Diagnosis |
Key distinguishing features |
Common organisms |
Initial antibiotic treatment |
|
RPA |
|
Polymicrobial: Group A streptococcus (S. pyogenes), S. aureus, respiratory anaerobes |
Ampicillin-sulbactam or clindamycin |
|
PTA |
|
|
Ampicillin-sulbactam or clindamycin |
|
Bacterial tracheitis |
|
|
IV broad-spectrum antibiotics to include MRSA (e.g., cefepime and vancomycin) |
References:
- Li RM, Kiemeney M. Infections of the neck. Emerg Med Clin North Am. 2019;37(1):95-107. PMID: 30454783. doi:10.1016/j.emc.2018.09.003
- Akhavan M. Ear, nose, throat: beyond pharyngitis: retropharyngeal abscess, peritonsillar abscess, epiglottitis, bacterial tracheitis, and postoperative tonsillectomy. Emerg Med Clin North Am. 2021;39(3):661-675. Published online June 9, 2021. PMID: 34215408. doi: 10.1016/j.emc.2021.04.012
- Woods CR, Cash ED, Smith AM, et al. Retropharyngeal and parapharyngeal abscesses among children and adolescents in the United States: epidemiology and management trends, 2003-2012. J Pediatric Infect Dis Soc. 2016;5(3):259-268. Published online March 22, 2015. PMID: 26407249. doi:10.1093/jpids/piv010
- Ungkanont K, Yellon RF, Weissman JL, Casselbrant ML, González-Valdepeña H, Bluestone CD. Head and neck space infections in infants and children. Otolaryngol Head Neck Surg. 1995;112(3):375-382. PMID: 7870436. doi:10.1016/s0194-5998(95)70270-9
- Salamone FN, Bobbitt DB, Myer CM, Rutter MJ, Greinwald JH Jr. Bacterial tracheitis reexamined: is there a less severe manifestation? Otolaryngol Head Neck Surg. 2004;131(6):871-876. PMID: 15577783. doi:10.1016/j.otohns.2004.06.708