Spine Stabilization Guidance
In patients with spinal cord injury, with or without radiographic abnormality, maintaining restriction of spinal motion is imperative to preserve and protect the spinal cord. The following segments include education pieces consistent with nursing interventions for the pediatric spinal cord injury patient.
Cervical Spine Stabilization
C-Collar Precautions
-
Keep C-Collar on until cleared by spine team (Trauma, Neurosurgery, Orthopedic Surgery)
-
Check skin under the collar every shift
-
Use moisture-wicking foam (e.g., thick white Mepilex) to pad friction areas
-
-
C-collar removal requires 2 staff members for safety and stability
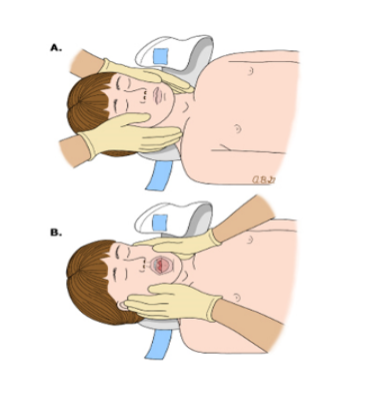
Manual Stabilization (No C-Collar)
-
Provider places hands on both sides of the head (A)
-
Fingertips gently touch the clavicles to prevent movement (A)
Important Notes
-
Use rigid cervical collars only for motion restriction
Head and Spine Alignment
- A Certified Trauma Nursing Core Course (TNCC)/Trauma Intensive Care Unit (TICU) nurse may hold cervical spine
- Keep head in neutral, midline position
- Use gel pillows, Z-flow, or sandbags for support
- Keep head of bed at 150 or use reverse Trendelenburg unless ordered otherwise
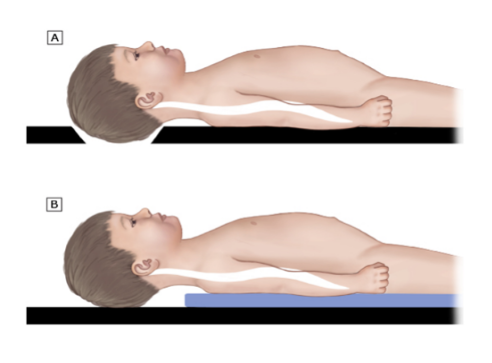
- For children under 8 years:
- Use 2 cm padding under head/neck
- Ensure occiput recess in bed/board (A)
- Add padding under shoulders, trunk, and legs (B)
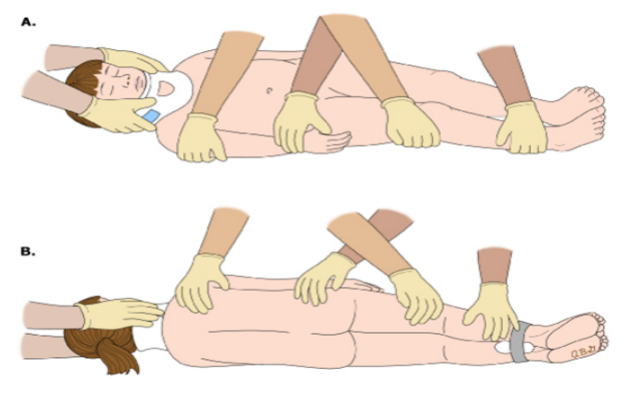
Repositioning Guidelines
- Log roll every 2 hours with at least 3 staff members
- A TNCC/TICU-certified nurse must stabilize the cervical spine
- Staff should interlock arms at the waist for proper technique (A. & B.)
- Ensure support staff are present for:
- Hygiene care
- Sheet changes
- Airway management (especially if intubated)
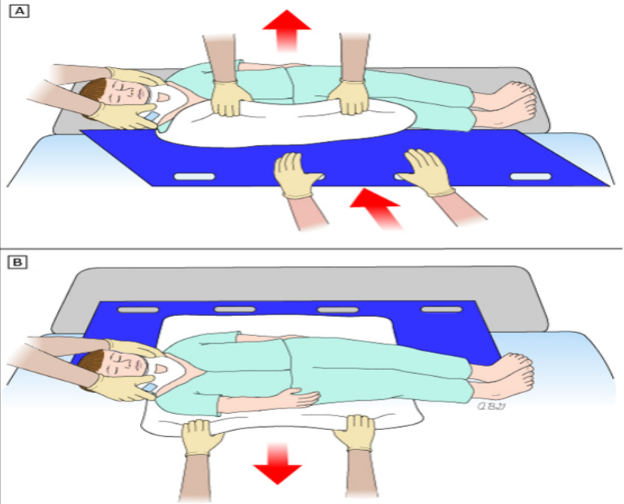
- Be cautious of lines, tubes, and drains during movement
- Use a Sally Tube for safe transfers between surfaces to maintain alignment (A & B)
These pathways do not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the patient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare a pathway for each. Accordingly, these pathways should guide care with the understanding that departures from them may be required at times.