Wise Use of Antibiotics: Using Your Village: How Antimicrobial Stewardship Collaboratives Benefit Everyone
We’ve all heard the adage “it takes a village to raise a child.” Antimicrobial stewardship collaboratives apply this same principle of using a “village” to achieve their goals. Improving judicious antimicrobial use is not something any one clinician, clinic or hospital can accomplish alone. Just as children benefit from the collective strengths of their community, the impact of stewardship efforts increases when individuals from different clinical settings and locations join forces.
Examples of Successful Antimicrobial Stewardship Collaborations
For more than a decade, the American Academy of Pediatrics (AAP) has sponsored national antimicrobial stewardship collaboratives through various Quality Networks across multiple clinical settings. The Reducing Variability in Infant Sepsis Evaluation (REVISE) collaborative included ≥ 100 hospitals and 20,000 infants. While empiric antibiotic use did not improve, the collaborative improved hospital utilization and length of stay for low-risk febrile infants.1 REVISE II built on this work by emphasizing adherence to the AAP’s new clinical pathway for well-appearing febrile infants ages 8 to 60 days.2 REVISE II reduced the empiric antibiotic duration, lumbar punctures and hospital admissions for low-risk patients.3 The Better Antibiotic Selection in Children (BASiC) collaborative demonstrated improvements across multiple inpatient and emergency department metrics including empiric use of antibiotics (67% to 72%), selection of preferred antibiotic agent (74% to 79%) and recommended treatment duration (61% to 71%).4 Similarly, the Improving Prescribing Antibiotics for Children in Urgent Care (IPAC in UC) collaborative increased the use of safety‑net antibiotic prescriptions for non‑severe acute otitis media and promoted appropriate testing prior to treating group A streptococcal pharyngitis.5
The AAP has also supported regional antimicrobial stewardship collaboratives using state chapter quality networks, often in partnership with state and federal health agencies.6,7 The Virginia Chapter Quality Network also engaged Anthem Blue Cross Blue Shield’s Enhanced Personal Health Care program (EPHC) to offer shared savings to enrolled clinicians who met quality metrics during the collaborative.6
Beyond the AAP, the Pediatric Infectious Diseases Society sponsors the Sharing Antimicrobial Reports for Pediatric Stewardship – Outpatient (SHARPS-OP) collaborative. SHARPS-OP includes outpatient antimicrobial stewardship champions from a variety of backgrounds including primary care, emergency medicine, urgent care, infectious diseases, pharmacy and epidemiology. Through data sharing and monthly webinars, the collaborative focuses on implementing best practices in diagnostic stewardship and judicious antibiotic use.8,9
What Participation Looks Like
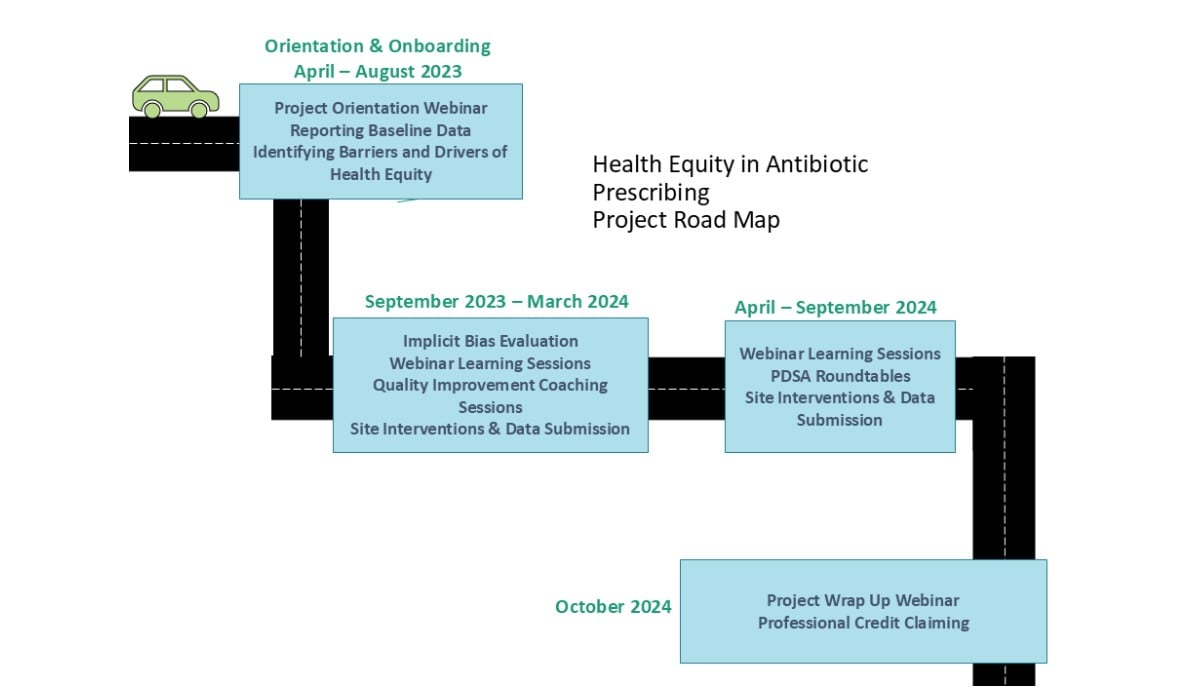
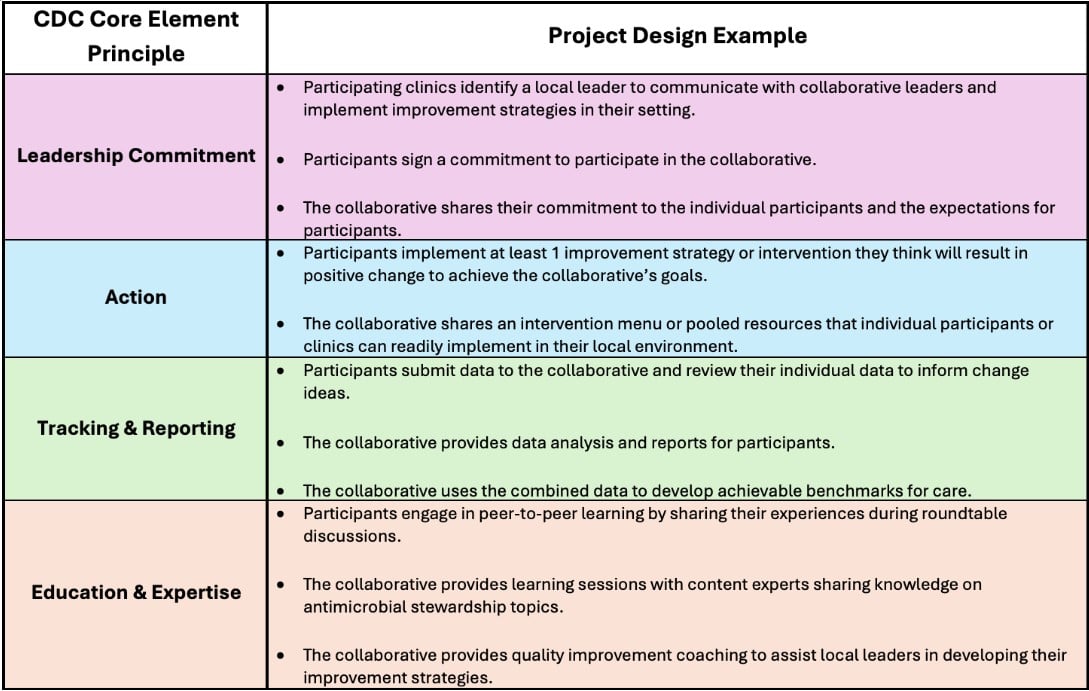
Although each antimicrobial stewardship collaborative is unique, most use the Centers for Disease Control and Prevention’s Core Elements of Outpatient Antimicrobial Stewardship as a framework10 (Table 1). Many follow the Institute for Healthcare Improvement’s Collaborative Model for Breakthrough Improvement incorporating learning sessions and iterative Plan-Do-Study-Act (PDSA) cycles during action periods11 (Figure 1). While participation requires a commitment to meaningful engagement, the typical time commitment is only a few hours a month.
How Collaboratives Strengthen Individuals
Participants overwhelmingly report peer-to-peer networking as the most valuable aspect of collaboratives.5 Additional benefits include access to data support, high-quality educational content and shared resources, including order sets, communication scripts, family education materials and clinical decision aids. By pooling resources and strategies, participants can more efficiently implement readily available improvements in their local settings. Many collaboratives also offer professional credit opportunities that support board certification requirements.
How Individuals Strengthen Collaboratives
While developing and leading a collaborative requires significant time and resources, sponsoring organizations and collaborative leaders recognize the value of implementing improvement strategies and learning from diverse clinical settings. Additionally, participants contribute real-world experience that helps identify barriers, refine strategies, and spark innovation and improvement that may not emerge without these varied perspectives. Finally, collaboratives benefit when individuals take lessons learned back to their local communities and share them with their colleagues. This creates a ripple effect that amplifies and strengthens the collaborative’s efforts beyond the initial collaborative.
Joining an Antibiotic Stewardship Village
If you are interested in getting involved, consider connecting with the Children’s Mercy Antimicrobial Stewardship Program (ASP). The ASP team (AntimicrobialStewards@cmh.edu) offers multiple opportunities to engage in outpatient antimicrobial stewardship initiatives, collaborate on improvement projects, share data and co-develop practical tools that support judicious antibiotic use. They are excited to explore partnership opportunities with clinicians across a variety of care settings.
Health care professionals face an increasingly complex prescribing landscape as telehealth expands, antibiotic shortages persist and resistance patterns evolve. National collaboratives offer a way to stay ahead of these challenges through shared knowledge, pooled resources and community support. Each new participant strengthens the network and expands the impact. Together, this village of antibiotic stewardship champions can achieve far more than any individual, clinic or hospital working alone.
References:
- Biondi EA, McCulloh R, Staggs VS, et al. Reducing Variability in the Infant Sepsis Evaluation (REVISE): a national quality initiative. Pediatrics. 2019;144(3):e20182201.
- Pantell RH, Roberts KB, Adams WG, et al. Evaluation and management of well-appearing febrile infants 8 to 60 days old. Pediatrics. 2021;148(2):e2021052228.
- McDaniel CE, Kerns E, Jennings B, et al. Improving guideline-concordant care for febrile infants through a quality improvement initiative. Pediatrics. 2024;153(5):e2023063339.
- McCulloh RJ, Kerns E, Flores R, et al. A national quality improvement collaborative to improve antibiotic use in pediatric infections. Pediatrics. 2024;153(5):e2023062246.
- Monti J, Jennings B, Schissel M, McKinsey J, El Feghaly RE, Nedved A. A learning collaborative to improve antibiotic use for otitis media and pharyngitis in pediatric urgent care clinics. Pediatr Emerg Care. 2025;41(12):e218-e226.
- Norlin C, Fleming-Dutra K, Mapp J, et al. A learning collaborative to improve antibiotic prescribing in primary care pediatric practices. Clin Pediatr (Phila). 2021;60(4-5):230-240.
- Frost HM, Monti JD, Andersen LM, et al. Improving delayed antibiotic prescribing for acute otitis media. Pediatrics. 2021;147(6):e2020026062.
- El Feghaly RE, Monsees EA, Burns A, et al. Outpatient antimicrobial stewardship programs in pediatric institutions in 2020: status, needs, barriers. Infect Control Hosp Epidemiol. 2022;43(10):1396-1402.
- El Feghaly RE, Herigon JC, Kronman MP, et al. Benchmarking of outpatient pediatric antibiotic prescribing: results of a multicenter collaborative. J Pediatric Infect Dis Soc. 2023;12(6):364-371.
- Sanchez GV, Fleming-Dutra KE, Roberts RM, Hicks LA. Core elements of outpatient antibiotic stewardship. MMWR Recomm Rep. 2016;65(6):1-12.
- The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement. Institute for Healthcare Improvement; 2003. https://www.ihi.org/library/white-papers/breakthrough-series-ihis-collaborative-model-achieving-breakthrough
Director, Quality Improvement, Urgent Care; Medical Director, Blue Valley Urgent Care; Professor of Pediatrics, University of Missouri-Kansas City School of Medicine; Clinical Assistant Professor of Pediatrics, University of Kansas School of Medicine
Director, Quality & Safety; Director, Outpatient Antimicrobial Stewardship Program; Director, Infectious Diseases Clinical Services; Medical Director, Vaccines for Children (VFC) Program; Professor of Pediatrics, University of Missouri-Kansas City School of Medicine; Clinical Assistant Professor of Pediatrics, University of Kansas School of Medicine