Evidence Based Strategies: Of Wax and Wayward Objects: Best Practices for Averting Shakespearean Tragedies in the Pediatric Ear Canal
Prologue
Friends, physicians, advanced practice providers, lend me your ears...
On the humble stage of the external auditory canal (EAC), two dramas unfold: cerumen impaction and ear foreign bodies. Though these players appear innocuous, they possess the capacity to cause chaos most foul. Thus, Children’s Mercy crafted two clinical pathways: Cerumen Impaction and Foreign Body - Ear. Both conditions alike in dignity, but each requiring slightly different approaches. Pray, read on to learn our recommendations for approaching these matters small in stature but oft perplexing in nature.
Much Ado About Ear Wax
Cerumen, or ear wax, acts as a self-cleaning agent in the EAC. There, it ensnares bacteria, dust and other debris. Chewing, reciting soliloquies in iambic pentameter, and other jaw movements promote transport of cerumen toward the ear opening where it dries and exits stage left.1 When this noble mechanism falters, cerumen may become impacted, obstructing the natural procession within the EAC and giving rise to mischief. Physiologic causes for cerumen impaction include anatomic anomalies of the ear, excessive cerumen production, and molecular changes in the viscosity of the cerumen.2 Objects in the EAC such as hearing aids, earbuds or other foreign interlopers may also inhibit the natural progression of cerumen. Although well intended, inserting cotton swabs or other cleaning devices into the EAC can worsen impaction by pushing cerumen deeper into the canal. Thus, the American Academy of Otolaryngology – Head and Neck Surgery cautions against placing any object in the EAC.1
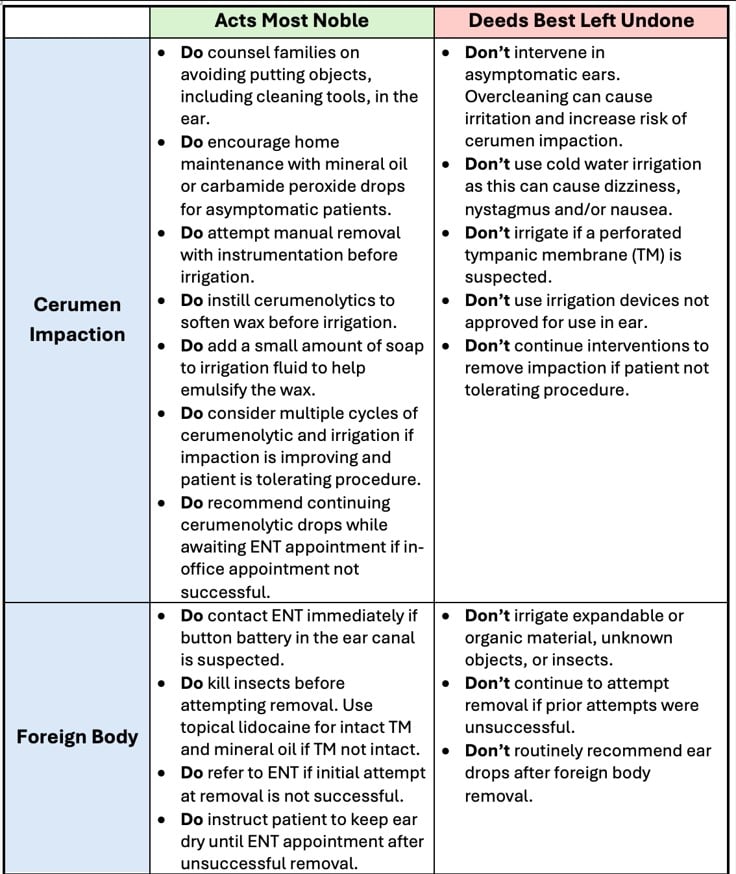
Often, cerumen impaction does not cause any symptoms and reveals itself only upon routine exam. Asymptomatic cases require no in-office intervention. Management should focus on at-home maintenance to prevent cerumen accumulation with carbamide peroxide (Debrox) or mineral oil drops. Yet, when troublesome symptoms of cerumen impaction arise (e.g., pain, feeling of pressure or fullness in the ear, ringing in the ear, hearing loss or dizziness), physicians and advanced practice providers should attempt manual extraction with instrumentation prior to using other methods of removal. If manual attempts yield unsuccessful results, instilling half-strength hydrogen peroxide, or other cerumenolytic, in the ear for five minutes may soften the adversary, allowing warm soapy water irrigation to carry the day. Soap emulsifies the wax and can make irrigation more effective. Successful removal may require multiple cycles of instilling the cerumenolytic and irrigating with lukewarm soapy water (Table 1).
Forsooth, as in all good comedies, know when to exit the stage. If the patient does not tolerate the procedure or the wax refuses to yield, discontinuing attempts at removal and referring to Otolaryngology (ENT) is the wiser course. Patients may continue at-home cerumenolytics in the days preceding their ENT appointment. Additional helpful tips for cerumen removal can be found here: Cerumen Impaction - Children's Mercy.
Ear Foreign Bodies: To Bead or Not to Bead...
That is the question curious children may ask themselves as they ponder what treasures to store in their tiny ear canal. The ear canal is the most common location for foreign bodies.3 Symptoms present similarly to those of cerumen impaction. Manual instrumentation, low suction (100-140 mmHg) with mushroom tip, and irrigation with lukewarm water may prove useful for extraction; yet the material dictates the method (Table 1).
- Button battery – A villain most dire due to its caustic power that can erode tissue within hours. Contact ENT at once.
- Live insects – Instill solution to kill the insect. For intact tympanic membranes (TM), topical lidocaine can be used. For patients with tympanostomy tubes or perforated TM, use mineral oil. Remove with instrumentation or suction.
- Expandable or organic material – Do not irrigate. Irrigation risks expanding the object. When in doubt, treat as expandable.
Other considerations may influence the approach to removal, including shape, location of the object, and prior failed attempts. Multiple in-office attempts with irrigation and instruments can lodge the object further in the canal and necessitate a surgical procedure for removal.4 Therefore, when the first attempt fails, refer to ENT before complications take center stage. More information on management of foreign bodies in the ear can be found here: Ear Foreign Body - Children's Mercy.
Epilogue
Thus concludes our tale of wax and wayward objects. This work was shaped by many players. We extend our sincere thanks to Gretchen Range, BSN, RN, CPN, Sheri Pratt, BSN, RN, CPN, and the Children’s Mercy Professional Governance Council for setting this effort in motion, and to all the contributing specialists whose expertise brought these clinical pathways to life. With these pathways as trusted guides, good healers can approach these conditions armed with reason, restraint and the knowledge that while we all strive to play the triumphant hero, sometimes the bravest deed is knowing when not to act and letting ENT take the stage.
References:
- Schwartz, SR, Magit AE, Rosenfeld RM, et al. Clinical practice guideline (update): earwax (cerumen impaction). Otolaryngol Head Neck Surg. 2017;156(1_suppl):S1-S29.
- Guest JF, Greener MJ, Robinson AC, Smith AF. Impacted cerumen: composition, production, epidemiology and management, 2004;97(8):477-488.
- Parajuli R. Foreign bodies in the ear, nose and throat: an experience in a tertiary care hospital in central Nepal. Int Arch Otorhinolaryngol. 2015;19(2):121-123.
- Curry SD, Maxwell AK. Management of foreign bodies in the ear canal. Otolaryngol Clin North Am. 2023;56(5):881-889.
Director, Quality Improvement, Urgent Care; Medical Director, Blue Valley Urgent Care; Professor of Pediatrics, University of Missouri-Kansas City School of Medicine; Clinical Assistant Professor of Pediatrics, University of Kansas School of Medicine
Clinical Assistant Professor of Pediatrics, University of Missouri-Kansas City School of Medicine; Education Assistant Professor of Pediatrics, University of Kansas School of Medicine
Medical Director, Office of Evidence-Based Practice; Associate Professor of Pediatrics, University of Missouri-Kansas City School of Medicine; Clinical Assistant Professor of Pediatrics, University of Kansas School of Medicine