Evidence-Based Strategies for Common Clinical Questions
March 2021
The Pressure is Rising: The Urgency of Addressing Pediatric Hypertension
Author: Charles Malloy, DO | Resident Physician of Medicine-Pediatrics

Column Editor: Kathleen Berg, MD | Pediatric Hospitalist, Division of Pediatric Hospital Medicine | Clinical Assistant Professor of Pediatrics, UMKC School of Medicine
Hypertension has long held the moniker “the silent killer” due to its well-known status as a risk factor for cardiovascular complications. While traditionally thought of as an adult problem, its prevalence in childhood and young adulthood warrants the attention of primary care pediatricians. Hypertension is very common in adults, with a prevalence of up to 40%.1 Longstanding elevated blood pressure causes left ventricular hypertrophy (LVH), arterial thickening, increased arterial stiffness, and decreased endothelial function.2 These in turn lead to increased cardiovascular disease, multi-vessel coronary artery disease, major adverse cardiac events, and all-cause mortality, even in adults 18-40 years of age.3,4,5
In children and adolescents, elevated blood pressure is predictive of hypertension and metabolic syndrome in adulthood.6 Higher systolic and diastolic pressures in children correlate with diastolic dysfunction when assessed with advanced echocardiographic techniques.7 LVH in young adulthood, a common consequence of pediatric hypertension, correlates with worse systolic function in middle age.8 End-stage renal disease, a feared complication of adult hypertension, occurs nearly twice as frequently in those who had hypertension as adolescents.9 Pediatric hypertension inversely correlates with scoring on tests of neurocognitive functions including attention, working memory, executive function and fine motor skills. Even children as young as 6-16 years of age performed worse on neurocognitive tests than matched children without hypertension.10 These effects could be lasting, as early hypertension also correlates with worse memory and visuospatial learning in adulthood.11
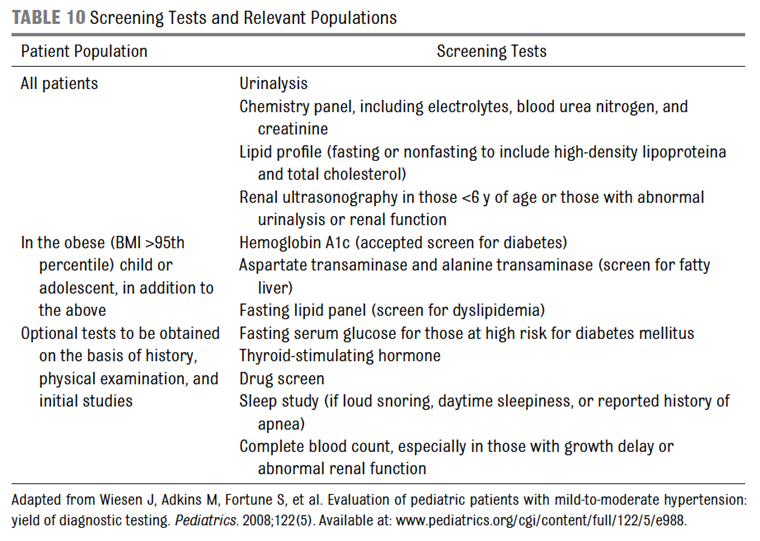
To combat the increasing prevalence of end-organ damage, the American Academy of Pediatrics (AAP) published an updated clinical practice guideline for the diagnosis and management of pediatric hypertension in 2017.12 New data in the adult literature led to the American Heart Association lowering the cutoff for the diagnosis of hypertension. Following suit, the AAP lowered the cutoffs for elevated blood pressure and hypertension in the updated guideline. The AAP also provided streamlined and thorough recommendations for the initial work-up of newly diagnosed elevated blood pressure or hypertension (Figure 1).13 These recommendations include close follow-up within one month after initial diagnosis of hypertension and within six months of elevated blood pressure. If blood pressure is still elevated at the specified duration, the AAP recommends laboratory evaluation, ambulatory blood pressure monitoring, and subspecialty referral. The initial work-up is detailed in Figure 2.12 When considering pharmacologic therapy, an echocardiogram is recommended as presence of left ventricular dysfunction is one indication for antihypertensive initiation.
Initial lifestyle interventions should be initiated for all children with elevated blood pressure or hypertension.12 Dietary Approaches to Stop Hypertension (DASH) diet education and at least 40 minutes of moderate exercise three to five times per week are recommended. Motivational interviewing should be implemented to increase application of these recommendations. Mindfulness exercises and other stress reducers are beneficial as adjunctive therapy. Pharmacologic therapy should begin when lifestyle modifications have not lowered blood pressure sufficiently at the specified follow-up interval, left ventricular hypertrophy is noted on echocardiogram, hypertensive symptoms occur, or if a patient has stage 2 hypertension without a modifiable risk factor. Angiotensin converting enzyme inhibitors/angiotensin receptor blockers, calcium channel blockers, and thiazide diuretics are first-line therapeutics.
The 2017 AAP guideline is superior to its 2004 guideline in predicting adult hypertension and metabolic syndrome.14 However, evidence suggests suboptimal implementation of the guideline. In a retrospective study of over 60,000 children, 10% had at least one abnormal blood pressure. Almost 60% of those with hypertension and 80% of those with prehypertension did not have diagnoses noted in their charts. Additionally, only 13% and 41% of these children had the recommended follow-up at one month and six months, respectively.15 With an estimated U.S. prevalence of pediatric hypertension of 4%, which is likely underestimated due to the delayed diagnosis, the potential impact of missed diagnosis and intervention is quite large.16
The prevalence of pediatric hypertension currently outstrips subspecialist availability in most communities.17 Therefore, primary care providers are tasked with the initial diagnosis, work-up, and management of those with elevated blood pressure and hypertension. We, as pediatricians, have a vital role in preventing end-organ damage due to hypertension, which includes not only cardiovascular and renal, but also neurocognitive sequelae. We must stay abreast of evolving evidence so that we may better optimize children’s short- and long-term outcomes.
Figure 1: Follow-up schedule for elevated blood pressure and stages 1 and 2 hypertension13
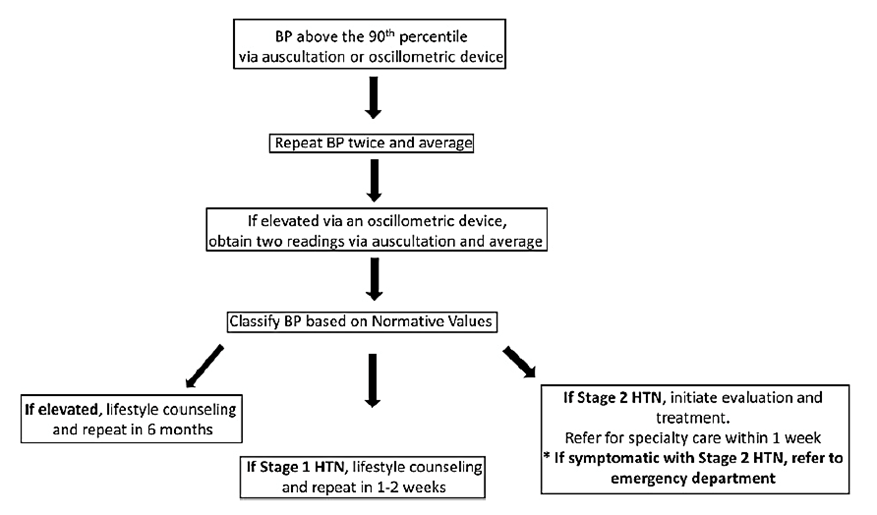
Figure 2: Initial laboratory work-up for new diagnosis of hypertension13
References:
- Chow CK, Teo KK, Rangarajan S, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013 Sept 4;310(9):959-968. doi:10.1001/jama.2013.184182.
- Khoury M, Urbina EM. Cardiac and vascular target organ damage in pediatric hypertension. Front Pediatr. 2018 May 24;6:148. doi: 10.3389/fped.2018.00148.
- Ge J, Li J, Yu H, Hou B. Hypertension is an independent predictor of multivessel coronary artery disease in young adults with acute coronary syndrome. Int J Hypertens. 2018 Nov 13;2018:7623639. doi:10.1155/2018/7623639.
- Yano Y, Reis JP, Colangelo LA, et al. Association of blood pressure classification in young adults using the 2017 American College of Cardiology/American Heart Association blood pressure guideline with cardiovascular events later in life. JAMA. 2018 Nov 6;320(17):1774-1782. doi: 10.1001/jama.2018.13551.
- Miura K, Daviglus ML, Dyer AR, et al. Relationship of blood pressure to 25-year mortality due to coronary heart disease, cardiovascular diseases, and all causes in young adult men: the Chicago Heart Association Detection Project in Industry. Arch Intern Med. 2001 Jun 25;161(12):1501-1508. doi: 10.1001/archinte.161.12.1501.
- Sun SS, Grave GD, Siervogel RM, Pickoff AA, Arslanian SS, Daniels SR. Systolic blood pressure in childhood predicts hypertension and metabolic syndrome later in life. Pediatr. 2007 Feb;119(2):237-246. doi:10.1542/peds.2006-2543.
- Navarini S, Bellsham-Revell H, Chubb H, Gu H, Sinha MD, Simpson JM. Myocardial deformation measured by 3-dimensional speckle tracking in children and adolescents with systemic arterial hypertension. Hypertension. 2017 Dec;70(6):1142-1147. doi:10.1161/HYPERTENSIONAHA.117.09574.
- Kishi S, Armstrong AC, Gidding SS, Jacobs DR Jr, Sidney S, Lewis CE, Schreiner PJ, Liu K, Lima JA. Relation of left ventricular mass at age 23 to 35 years to global left ventricular systolic function 20 years later (from the Coronary Artery Risk Development in Young Adults study). Am J Cardiol. 2014 Jan 15;113(2):377-83. doi: 10.1016/j.amjcard.2013.08.052.
- Leiba A, Fishman B, Twig G, et al. Association of adolescent hypertension with future end-stage renal disease. JAMA Intern Med. 2019 Apr 1;179(4):517-523. doi:10.1001/jamainternmed.2018.7632.
- Lande MB, Batisky DL, Kupferman JC, et al. Neurocognitive function in children with primary hypertension. J Pediatr. 2017 Jan;180:148-155.e1. doi:10.1016/j.jpeds.2016.08.076.
- Rovio SP, Pahkala K, Nevalainen J, et al. Cardiovascular risk factors from childhood and midlife cognitive performance: The Young Finns Study. J Am Coll Cardiol. 2017 May 9;69(18):2279-2289. Doi:10.1016/j.jacc.2017.02.060.
- Flynn JT, Kaelber DC, Baker-Smith CM, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017 Sep;140(3):e20171904. doi:10.1542/peds.2017-1904.
- Weaver DJ Jr. Pediatric Hypertension: Review of updated guidelines. Pediatr Rev. 2019 Jul;40(7):354-358. Doi:10.1542/pir.2018-0014.
- Du T, Fernandez C, Barshop R, Chen W, Urbina EM, Bazzano LA. 2017 pediatric hypertension guidelines improve prediction of adult cardiovascular outcomes. Hypertension. 2019 Jun;73(6):1217-1223. doi:10.1161/HYPERTENSIONAHA.118.12469.
- Moin A, Mohanty N, Tedla YG, et al. Under-recognition of pediatric hypertension diagnosis: Examination of 1 year of visits to community health centers. J Clin Hypertens (Greenwich). 2020 Dec 29;10.1111/jch.14148. doi:10.1111/jch.14148.
- Bell CS, Samuel JP, Samuels JA. Prevalence of hypertension in children. Hypertension. 2019 Jan;73(1):148-152. doi: 10.1161/HYPERTENSIONAHA.118.11673.
- Hill KD, Li JS. Childhood hypertension: an underappreciated epidemic? Pediatr. 2016 Dec;138(6):e20162857. doi:10.1542/peds.2016-2857.